Hypothyroidism, hyperglycemia and HUFA metabolism

Is sugar really the cause of diabetes or do fats and hormones have a role?
These are strange times in which we live. Apparently, there’s a virus that’s deadlier than the deaths attributed to hunger, pollution, stress and cancer. The latter deaths running into many tens of millions annually seems less important to consider at present. It appears analogous to the notion that people still think that sugar causes diabetes and cancer. The notion that total sugar restriction (like the current viral restrictions, also lacking in solid science) is the obvious answer to lowering hyperglycemic and diabetic states. It’s probably driven by the idea that “carbohydrates are not essential, as your body can make its own from gluconeogenesis (liberating energy from fats and proteins). Often ignoring the concept that complex organised physiology efficiently uses carbohydrates to produce energy, water and carbon dioxide without the need for activation of the stress hormone pathways.
The stressful world from which we have evolved from has been replaced by a new world, with new stressors that require maintenance of complex biology not increasing its degradation with simplistic, shortsighted solutions.
Popular interventions for those with metabolic disturbances include low carbohydrate diets, fasting or Omega 3s, ignoring the driving phenomenon for a more reduced yet superficially pleasing intervention. Two of my recent previous blogs expand on why fasting and fish oil appear useful on the surface but when you dig into the long term effects of decreased efficiency and metabolism, things don’t quite add up. The concept of taking fish oils or omega 3s for lowering blood glucose values is as reductionist and problematic as the suggestion of their lipid lowering effects. It’s a bit like fasting. Should you fast or do you even need to fast? Maintaining physiology at its best, and in an ever increasingly polluted and stressful environment is not always achieved with suppression and restriction.
Thyroid hormone controls glucose blood values, and hyperglycemia is a symptom of hypothyroidism. There must be an assumption that when you take omega 3s they must be able to resolve both subclinical and an overt hypothyroid state? The ability of the polyunsaturated oils, especially DHA to lower thyroid hormone receptor expression and has been known for decades to prevent binding of T3 to its receptor (INOUE et al., 1989)(van der Klis, Schmidt, van Beeren, & Wiersinga, 1991)
Disruptions to oxidative metabolism and the electron transport chain is mediated by pollution, stress, estrogen and high fat diets amongst others. The loss of energetic efficiency and utilisation of carbohydrates (to chronic fatty acid metabolism) can promote reductive metabolism where the ratio of the coenzymes NAD:NADH is decreased. To ensure that NADH is oxidised to enhance NAD recycling (REDOX potential – oxidation is loss, reduction is gain - or OIL RIG), highly unsaturated fatty acids (HUFA) are increased through the use of the desaturase enzymes 5 and delta 6 desaturase (W. et al., 2018). It’s helpful acutely to respond to diminished oxidation of carbohydrate and fatty acids but long term a driving force behind disease progression.
Chronic use of the desaturase enzymes promotes metabolic disease by further degrading oxidative metabolism from sustained glycolysis (used to recycle NAD;NADH inefficiently), shift to glycolysis, conversion of pyruvate to lactate and increased lipid peroxidation. This tends to support the research suggesting that the higher the level of tissue unsaturation the shorter the life span and vice versa (Hulbert, Kelly, & Abbott, 2014) (Hulbert, 2007).
Thyroid hormone permeates every level of complex physiology. Pancreatic function and glucose regulation are not an exception. Thyroid hormone receptors are found in both exocrine and endocrine components of the pancreas (Chen, Xie, Shen, & Xia, 2018). Thyroid hormone promotes pancreatic growth and differentiation. Hypothyroidism in mothers and inherited hypothyroid traits may lead to altered morphology and pancreatic function in offspring that predisposes offspring to diabetic states (Karbalaei, Ghasemi, Faraji, & Zahediasl, 2013; Päkkilä et al., 2013).
Inheritance, pollution and stress contribute to altered (detectable and undetectable) thyroid hormone assimilation and availability, thereby affecting pancreatic and glucose regulation. Consumption or restriction of carbohydrates in a system that is experiencing an aspect of metabolic inflexibility will have obvious consequences. Increased glucose values or decreased but that’s not set in stone and dependant on metabolic flexibility.
Restriction of sugar due to the inflexibility of the system seems the obvious choice but ignores the very question of why the hyperglycemia exists. I’ll concede that if all you ever eat is just pure sugar in the diet with nothing else, it may have merits. No one does this. Even commercial fast foods are replete with fats and proteins. Usually this issue is one of over consumption but that’s another subject. It’s very well known that high fat and calorie diets induce lipotoxicity and the accumulation of both unsaturated and saturated fats in many tissues like the brain and heart are a product of metabolic inflexibility and disease (Zhang et al., 2018) (Fecchio, Palazzi, & Polverino de Laureto, 2018). Saturated fats and their phospholipids tend to be more stable than the unsaturated fats yet still have an optimal level. Excess amounts can still be an issue.
Fasting, low carbohydrate and fish oil consumption have nice superficial appearance of lowering glucose levels, simply because carbohydrates are significantly decreased and or oxidation of fatty acids is enhanced. Therefore insulin need is less.
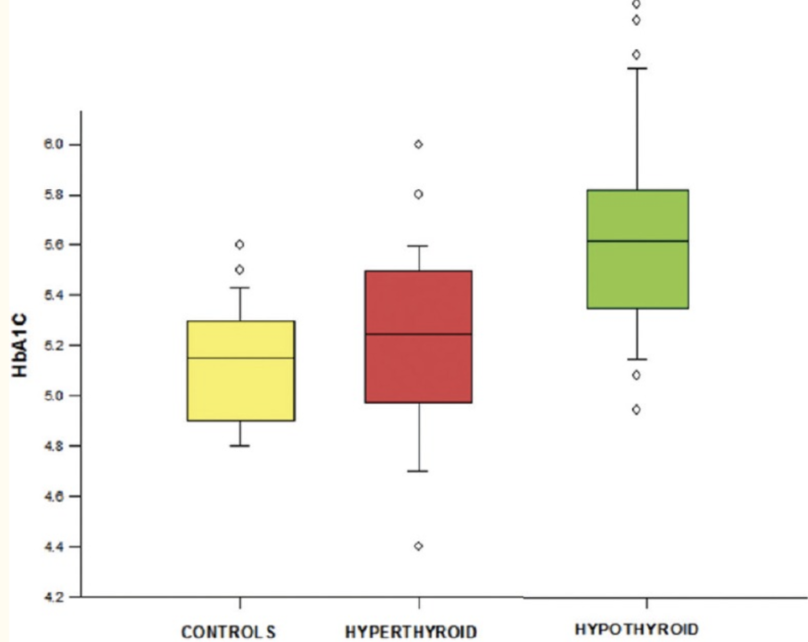
Glycation of hemoglobin or HBa1c test is used as a marker of efficient glucose use. It can be affected by hypothyroidism and made worse by chronic and incomplete oxidation of fatty acids.
.
Glycation of hemoglobin or HBa1c test is used as a marker of efficient glucose use. It can be affected by hypothyroidism and made worse by chronic and incomplete oxidation of fatty acids.
Thyroid autoimmunity and pancreatic dysfunction are well known but it’s a systemic issue not an immunity issue. The body is quite well suited for recognising self from non- self and therefore autoimmunity is unlikely to be anything more exciting than the body removing tissue for destruction (Matzinger, 2012)(Cunliffe, 1995). It’s well known that autoimmune tags like Hashimotos progress to overt hypothyroidism with increasing symptoms. Managing thyroid status beyond the context of blood tests may be suitable for lowering antibodies and avoiding potentially years of ever decreasing health of those who may suffer from a diagnosis of thyroid autoimmunity.
Many studies have shown that establishing normal thyroid function (euthyroid) is associated with reversing high cholesterol, blood pressure, fatty liver and glucose states (Roos, Bakker, Links, Gans, & Wolffenbuttel, 2007) (Gao, Zhang, Zhang, Yang, & Chen, 2013; Kim et al., 2018). Too often, studies that have failed to show a positive effect for synthetic T4 or Levothyroxine, are cited to show the unsuitability of restoring thyroid hormone to reverse these conditions (Surks, Goswami, & Daniels, 2005). Assumption that T4 as a stand-alone therapy is effective, should be consigned as dogmatic belief from endocrine text of the past. T4/T3, T3 alone or NDT (natural desiccated thyroid), individual stress, nutrition, pollutant exposure or emotional abuse are just some of the subjective nuances rarely taken into account for evaluating thyroid interventions. Additionally, the concept of normal TSH, T4 and T3 values from biochemistry analysis seems more problematic than ever (Peat, 1999).
If increasing Omega 3s for blood sugar issues is useful, what effect does it have on other aspects of function? Increasing DHA at the cell membrane promotes easily oxidised fuel sources, increasing the flip flop effect (oxidised head flips from outer to inner), makes membranes leakier yet less permeable to ions, and induces pryoptosis - an inflammatory form of programmed cell death (Fabre, Cerny, Cassen, & Mouloungui, 2018) (Herr et al., 2020). I think it’s one of the main reasons DHA is used to enhance the toxicity of chemotherapy.
Given that thyroid hormones promote membrane integrity, function as a membrane antioxidant, enhance oxidative metabolism and with specific reference, attenuate hyperglycaemia and pancreatic dysfunction. Perhaps a more rounded investigation into its assessment and subjective restrictions (type of hormone and individual’s environment) remains the most useful course of action? Cutting out, and worse still demonising sugars, at a time when the body requires less stress, not more, makes little sense.
References:
Bhattacharjee R, Thukral A, Chakraborty PP, et al. Effects of thyroid status on glycated hemoglobin. Indian J Endocrinol Metab. 2017;21(1):26-30. doi:10.4103/2230-8210.196017
Chen, C., Xie, Z., Shen, Y., & Xia, S. F. (2018). The roles of thyroid and thyroid hormone in pancreas: Physiology and pathology. International Journal of Endocrinology. https://doi.org/10.1155/2018/2861034
Cunliffe, J. (1995). Morphostasis and immunity. Medical Hypotheses. https://doi.org/10.1016/0306-9877(95)90076-4
Fabre, J.-F., Cerny, M., Cassen, A., & Mouloungui, Z. (2018). Effect of methylene blue on the formation of oxidized phospholipid vesicles. BioRxiv, 403634. https://doi.org/10.1101/403634
Fecchio, C., Palazzi, L., & Polverino de Laureto, P. (2018). α-Synuclein and polyunsaturated fatty acids: Molecular basis of the interaction and implication in neurodegeneration. Molecules. https://doi.org/10.3390/molecules23071531
Gao, N., Zhang, W., Zhang, Y., Yang, Q., & Chen, S. (2013). Carotid intima-media thickness in patients with subclinical hypothyroidism: A meta-analysis. Atherosclerosis, 227(1), 18–25. https://doi.org/10.1016/j.atherosclerosis.2012.10.070
Herr, D. R., Yam, T. Y. A., Tan, W. S. D., Koh, S. S., Wong, W. S. F., Ong, W. Y., & Chayaburakul, K. (2020). Ultrastructural Characteristics of DHA-Induced Pyroptosis. NeuroMolecular Medicine. https://doi.org/10.1007/s12017-019-08586-y
Hulbert, A. J. (2007). Membrane fatty acids as pacemakers of animal metabolism. In Lipids. https://doi.org/10.1007/s11745-007-3058-0
Hulbert, A. J., Kelly, M. A., & Abbott, S. K. (2014). Polyunsaturated fats, membrane lipids and animal longevity. Journal of Comparative Physiology B: Biochemical, Systemic, and Environmental Physiology. https://doi.org/10.1007/s00360-013-0786-8
INOUE, A., YAMAMOTO, N., MORISAWA, Y., UCHIMOTO, T., YUKIOKA, M., & MORISAWA, S. (1989). Unesterified long‐chain fatty acids inhibit thyroid hormone binding to the nuclear receptor: Solubilized receptor and the receptor in cultured cells. European Journal of Biochemistry. https://doi.org/10.1111/j.1432-1033.1989.tb21085.x
Karbalaei, N., Ghasemi, A., Faraji, F., & Zahediasl, S. (2013). Comparison of the effect of maternal hypothyroidism on carbohydrate metabolism in young and aged male offspring in rats. Scandinavian Journal of Clinical and Laboratory Investigation. https://doi.org/10.3109/00365513.2012.743164
Kim, D., Kim, W., Joo, S. K., Bae, J. M., Kim, J. H., & Ahmed, A. (2018). Subclinical Hypothyroidism and Low-Normal Thyroid Function Are Associated With Nonalcoholic Steatohepatitis and Fibrosis. Clinical Gastroenterology and Hepatology, 16(1), 123-131.e1. https://doi.org/10.1016/j.cgh.2017.08.014
Matzinger, P. (2012). The evolution of the danger theory. Expert Review of Clinical Immunology. https://doi.org/10.1586/eci.12.21
Päkkilä, F., Männistö, T., Surcel, H. M., Ruokonen, A., Bloigu, A., Pouta, A., … Suvanto, E. (2013). Maternal thyroid dysfunction during pregnancy and thyroid function of her child in adolescence. Journal of Clinical Endocrinology and Metabolism. https://doi.org/10.1210/jc.2012-2028
Peat, R. (1999). Thyroid Therapies, Confusion and Fraud. Retrieved from www.raypeat.com/articles/articles/thyroid.shtml
Roos, A., Bakker, S. J. L., Links, T. P., Gans, R. O. B., & Wolffenbuttel, B. H. R. (2007). Thyroid function is associated with components of the metabolic syndrome in euthyroid subjects. The Journal of Clinical Endocrinology and Metabolism, 92(2), 491–496. https://doi.org/10.1210/jc.2006-1718
Surks, M. I., Goswami, G., & Daniels, G. H. (2005). The thyrotropin reference range should remain unchanged. Journal of Clinical Endocrinology and Metabolism, 90(9), 5489–5496. https://doi.org/10.1210/jc.2005-0170
van der Klis, F. R. M., Schmidt, E. D. L., van Beeren, H. C., & Wiersinga, W. M. (1991). Competitive inhibition of T3 binding to α1 and β1 thyroid hormone receptors by fatty acids. Biochemical and Biophysical Research Communications. https://doi.org/10.1016/0006-291X(91)91919-4
W., K., J.C., F., A., D., S.B.R., J., C.B., C., & E.P., R. (2018). Polyunsaturated fatty acid desaturase-mediated NAD+ recycling permits ongoing glycolysis and cell proliferation. FASEB Journal.
Zhang, X., Chen, W., Shao, S., Xu, G., Song, Y., Xu, C., … Zhao, J. (2018). A High-Fat Diet Rich in Saturated and Mono-Unsaturated Fatty Acids Induces Disturbance of Thyroid Lipid Profile and Hypothyroxinemia in Male Rats. Molecular Nutrition and Food Research, 62(6). https://doi.org/10.1002/mnfr.201700599
Newer PostThyroid hormones and longevity
Older PostThe Commonality of Statins and Omega 3s– neurological degeneration.
Balanced Body Mindkeith@balancedbodymind.com
COPYRIGHT 2020 BALANCED BODY MIND